

Abstract
Background: The randomized PETHEMA/GEM phase III trial GEM05menos65 (www.clinicaltrials.gov NCT00461747) demonstrated that pretransplant induction therapy with VTD resulted in a significantly higher CR rate both, pretransplant and postransplant and in a significantly longer progression-free survival (PFS) when compared with thalidomide/dexamethasone (TD) and combination chemotherapy plus bortezomib (VBMCP/VBAD/B) (Rosiñol et al, Blood 2012). We report here the definitive results of the trial, ten years after the last patient was included.
Methods: From April 6, 2006 to August 5, 2009, 386 patients younger than 65 years with newly diagnosed symptomatic multiple myeloma (MM) were randomized to receive three different induction regimens: six 4-week cycles of TD (thalidomide 200 mg daily; dexamethasone 40 mg on days 1-4 and 9-12) vs. six 4-week cycles of VTD (TD at identical doses plus i.v. bortezomib 1.3 mg/m2 on days 1, 4, 8 and 11) vs. combination chemotherapy plus bortezomib (4 cycles of alternating VBMCP and VBAD chemotherapy followed by two cycles of i.v. bortezomib at the usual dose of 1.3 mg/m2 on days 1,4,8,11 every 3 weeks). The duration of the induction therapy was 24 weeks in all arms. All patients were planned to undergo ASCT with high-dose melphalan at 200 mg/m2 followed by maintenance therapy with thalidomide/bortezomib (TV) vs. thalidomide (T) vs. alfa-2b-interferon (alfa2-IFN) for 3 years. One-hundred and thirty patients were allocated to VTD, 127 to TD and 129 to VBMCP/VBAD/B. Seventy out of the 330 patients (21%) with cytogenetic studies had high-risk cytogenetics [t(4;14), t(14;16) and/or 17p deletion]. Patient characteristics at diagnosis and prognostic factors such as ISS, cytogenetics and maintenance arm were similarly distributed in the 3 arms.
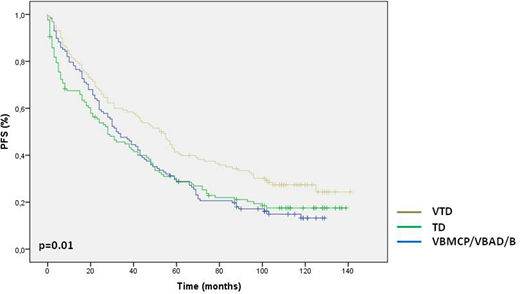
Results: After a median follow-up of 115 months for alive patients, VTD resulted in a significantly longer PFS when compared with TD and VBMCP/VBAD/B (52 vs 28 vs 32 months, p=0.01) (Figure 1). The median overall survival (OS) was 128 vs 99 vs 93 months, respectively, with no significant differences among the 3 arms.
In the overall series, the PFS was significantly shorter in patients with high-risk cytogenetics compared with patients with standard-risk (15 vs. 42 months, p=0.001). In the TD and in the VBMCP/VBAD/B arm patients with high-risk cytogenetics had a significantly shorter PFS than patients with standard-risk (7 vs 32 months, p=0.029 in TD group; 13 vs. 38 months, p=0.027 in VBMCP/VBAD/B group). However, there was no significant difference in the VTD arm (23 vs 52 months, p=0.125). Patients with high-risk cytogenetics had a significantly shorter OS in the overall series (median 38 months vs 114, p=0.0001) and this was observed in the three treatment arms: VTD median 36 months vs not reached (p=0.0001), TD median 52 months vs 113 (p=0.017), VBMCP/VBAD/B median 29 months vs 93 (p=0.01).
The achievement of a negative MRD after transplant was associated with a longer PFS and OS. Thus, on an intention to treat basis, patients who had MRD negative after transplant had a significantly longer PFS (59 vs 38 months, p=0.0001) and OS (median not reached vs 102 months, p=0.001) than those who remained MRD positive after ASCT. Of interest, there are no significant differences in PFS (41 months vs 60 months, p=0.367) or OS (114 moths vs not reached, p=0.329) between patients with high-risk or standard risk cytogenetics who achieved negative MRD after transplant.
By contrast, in patients with MRD positive after transplant, the PFS ( 16 months vs 38 months, p=0.006) and OS (29 months vs 113 months, p=0.001) was significantly shorter in patients with high-risk cytogenetics compared with patients with standard-risk cytogenetics.
Conclusions: Our long-term results confirm that induction with VTD results in a significantly longer PFS when compared with TD and VBMCP/VBAD/B. Patients with high-risk cytogenetics who achieved postransplant MRD negative had a similar outcome than patients with standard-risk cytogenetics, while patients with high-risk cytogenetics who remain MRD positive had a dismal prognosis. Finally, the PFS of 52 months achieved with VTD is the longest ever reported in the first line treatment of younger patients with MM elegible for ASCT and support the use of VTD as the standard of care for pretransplant induction therapy.
Rosinol Dachs:Amgen: Honoraria; Celgene: Honoraria; Janssen: Honoraria. Oriol:Amgen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Takeda: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Janssen: Consultancy, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Blanchard:Janssen: Honoraria. Granell:Janssen: Honoraria; Celgene: Honoraria. Mateos:GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees; Janssen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Celgene: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Abbvie: Consultancy, Membership on an entity's Board of Directors or advisory committees; Amgen: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; GSK: Consultancy, Membership on an entity's Board of Directors or advisory committees; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Martinez-Lopez:Celgene: Honoraria, Research Funding; Janssen: Honoraria, Research Funding; Vivia: Honoraria; Pfizer: Research Funding; BMS: Research Funding; Novartis: Research Funding. Alegre:Celgene: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; Amgen: Membership on an entity's Board of Directors or advisory committees; Janssen: Membership on an entity's Board of Directors or advisory committees. Lahuerta:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Takeda: Honoraria, Membership on an entity's Board of Directors or advisory committees; Amgen: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees. San-Miguel:BMS: Honoraria; Roche: Honoraria; Sanofi: Honoraria; Celgene: Honoraria; Amgen: Honoraria; Janssen: Honoraria; Novartis: Honoraria. Blade:Amgen: Honoraria; Celgene: Honoraria; Janssen: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal